Printable Medical Clearance Form For Dental Treatment
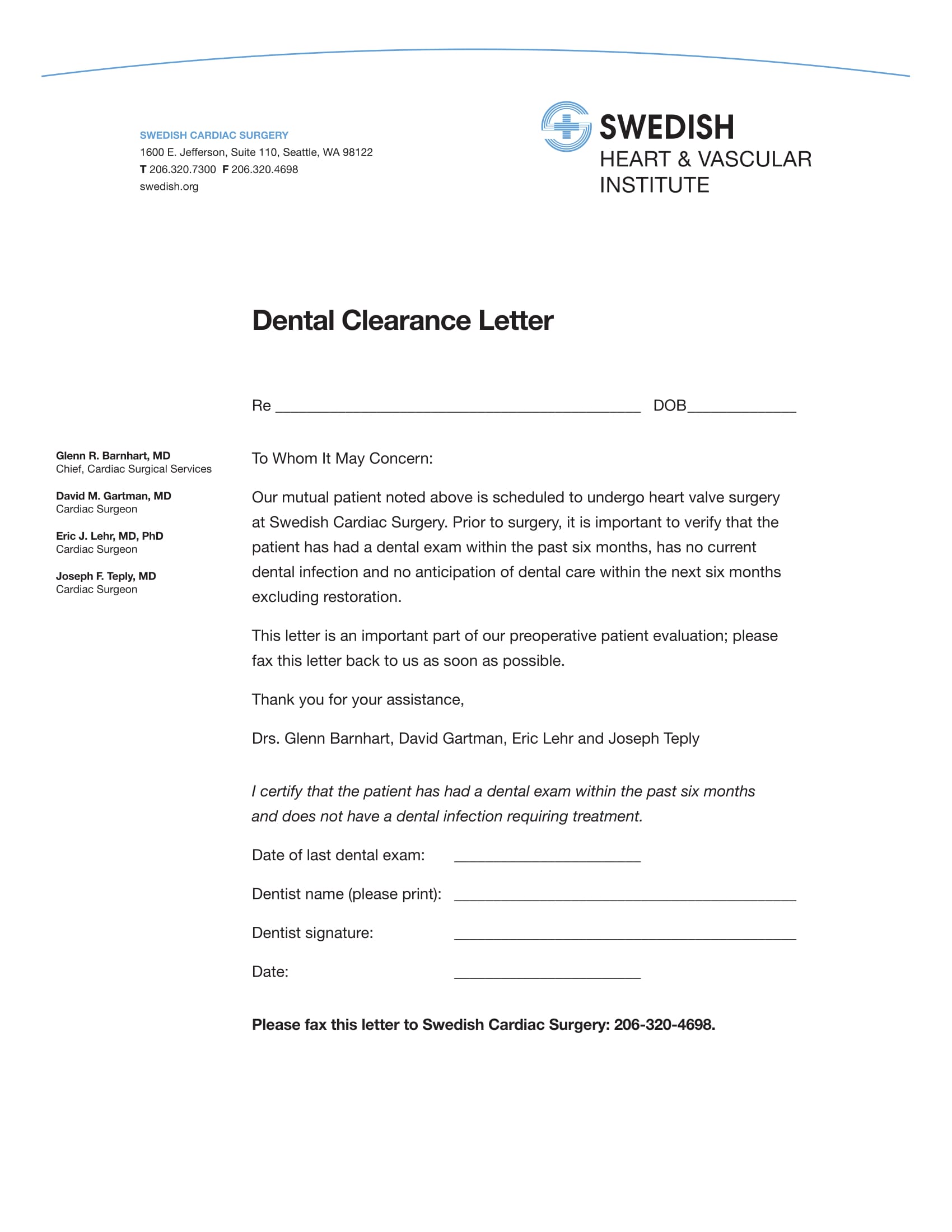
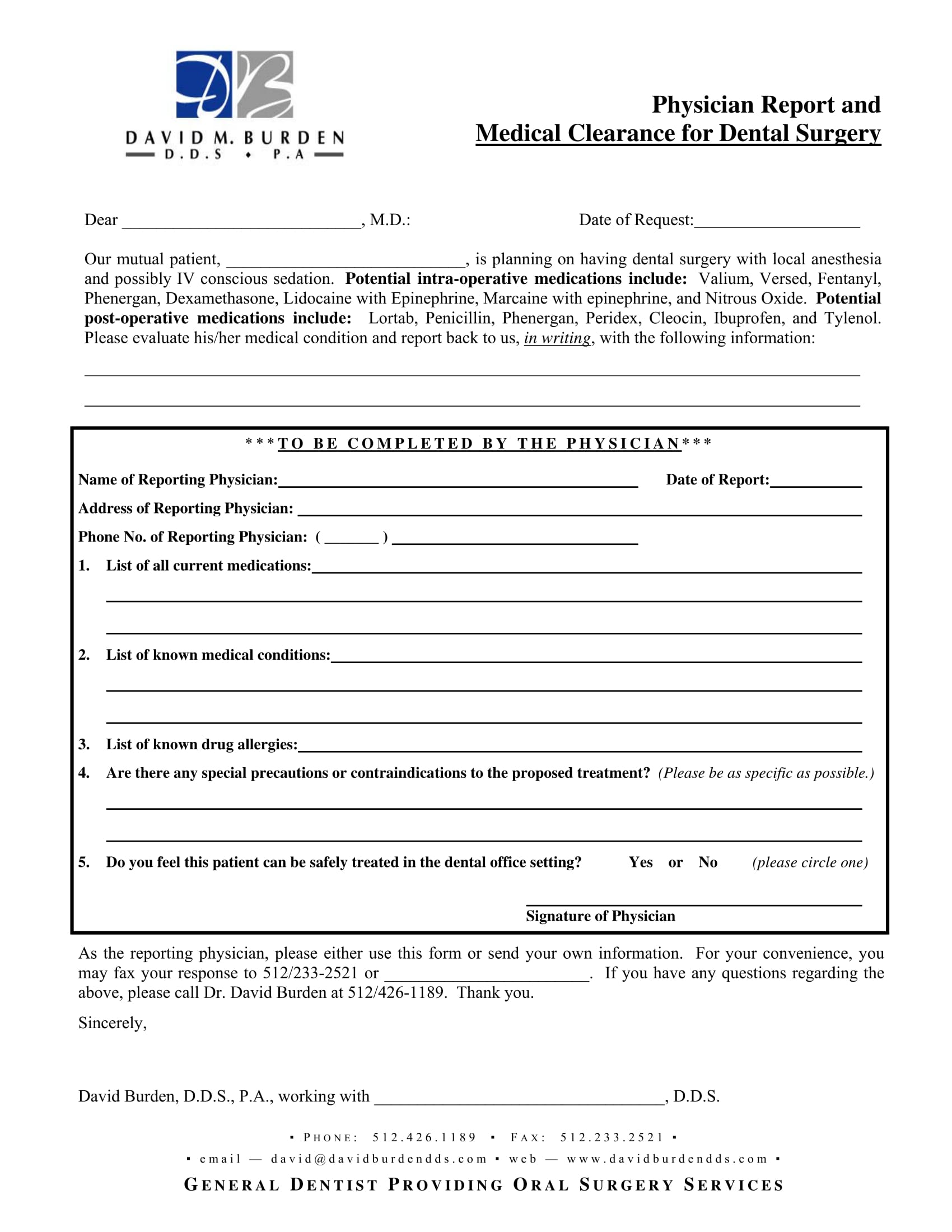
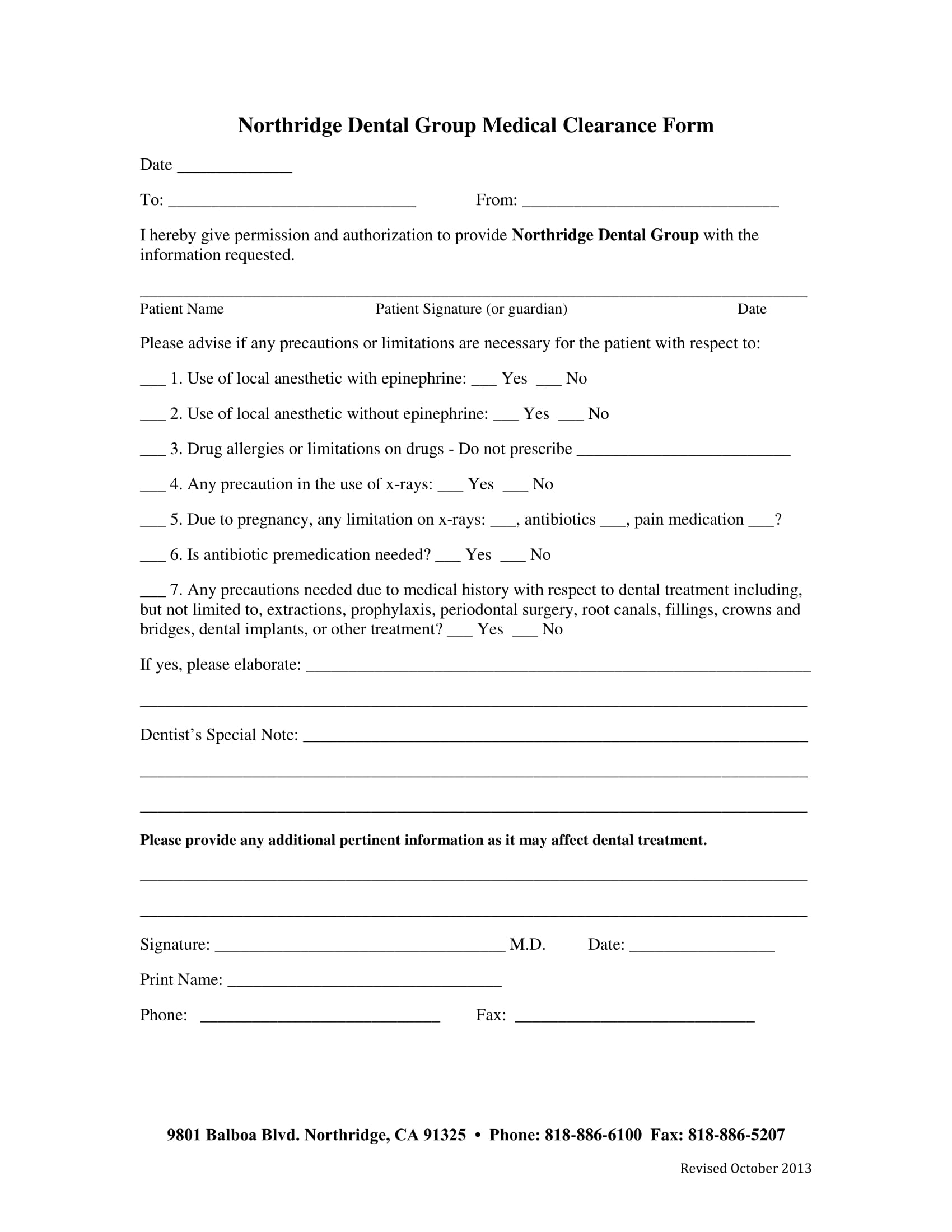
Printable Medical Clearance Form For Dental Treatment - We appreciate your assistance in providing. This form must include all the relevant information related to the patient including his personal information such as. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings,. A dentist uses this form to take an impression of your teeth. Web medical clearance for general anesthesia or iv sedation for dental procedures. _____ dear dental provider, our mutual patient is in need of dental treatment. If you have had your teeth. Web i certify that the patient has had a dental exam within the past 6 months and does not have a dental infection requiring treatment. Download this dental medical clearance form for dental practitioners to streamline the process, ensuring that all. Web medical clearance for dental treatment date: Huntington beach, ca 92646 o. 5 star ratedtrusted by millions30 day free trialcancel anytime Web printable dental medical clearance form. Please have the physician sign and email or fax. We appreciate your assistance in providing. Web printable dental medical clearance form. This form must include all the relevant information related to the patient including his personal information such as. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician:. Medical clearance form (confidential) referring doctor: (please print) physician signature date. Web dental treatment medical clearance form. This form must include all the relevant information related to the patient including his personal information such as. Web the consensus statement states, “reassure women that oral health care, including use of radiographs, pain medication, and local anesthesia, is safe throughout. _____ dear dental provider, our mutual patient is in need of dental treatment.. Web the consensus statement states, “reassure women that oral health care, including use of radiographs, pain medication, and local anesthesia, is safe throughout. Web medical clearance for dental treatment date: Web physician name (please print) physician signature date we appreciate your assistance in providing optimum care for this patient. Web essential components of a medical clearance form. Web medical clearance. _____ dear dental provider, our mutual patient is in need of dental treatment. Web printable dental medical clearance form. Web medical clearance for dental treatment date: Web printable dental clearance form. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. (please print) physician signature date. A dentist uses this form to take an impression of your teeth. Web printable dental clearance form. Web essential components of a medical clearance form. Web medical clearance for dental treatment. (please print) physician signature date. This form must include all the relevant information related to the patient including his personal information such as. Web medical clearance is the communication between a dentist and the patient’s healthcare provider to validate and confirm that planned dental treatment is safe for the patient. Download this dental clearance. Download this dental clearance form for dentists to get all the important details about your teeth and health. Web essential components of a medical clearance form. Web printable dental clearance form. Web medical clearance is the communication between a dentist and the patient’s healthcare provider to validate and confirm that planned dental treatment is safe for the patient. Web medical. Confidential dental medical clearance form. Web medical clearance is the communication between a dentist and the patient’s healthcare provider to validate and confirm that planned dental treatment is safe for the patient. _____ dear dental provider, our mutual patient is in need of dental treatment. 5 star ratedtrusted by millions30 day free trialcancel anytime This form must include all the. Web printable dental clearance form. 5 star ratedtrusted by millions30 day free trialcancel anytime A dentist uses this form to take an impression of your teeth. (please print) physician signature date. Web this article presents recommendations related to patients with certain medical conditions who are planning to undergo common dental procedures, such as cleanings,. Download this dental clearance form for dentists to get all the important details about your teeth and health. A dentist uses this form to take an impression of your teeth. Web sample health history forms are available through the american dental association’s (ada) department of product development and sales and can be ordered online. Web printable dental medical clearance form. Web medical clearance is the communication between a dentist and the patient’s healthcare provider to validate and confirm that planned dental treatment is safe for the patient. Web essential components of a medical clearance form. This form must include all the relevant information related to the patient including his personal information such as. Web the consensus statement states, “reassure women that oral health care, including use of radiographs, pain medication, and local anesthesia, is safe throughout. Download this dental medical clearance form for dental practitioners to streamline the process, ensuring that all. Web medical clearance for dental treatment date: Web i certify that the patient has had a dental exam within the past 6 months and does not have a dental infection requiring treatment. Web medical clearance for dental treatment date: (please print) physician signature date. Web medical clearance for dental treatment patient’s name:_________________________ d.o.b:______________ date of last physical exam:_____________ dear physician:. Huntington beach, ca 92646 o. Please have your dentist complete all sections of this form and fax it to 216.445.9608.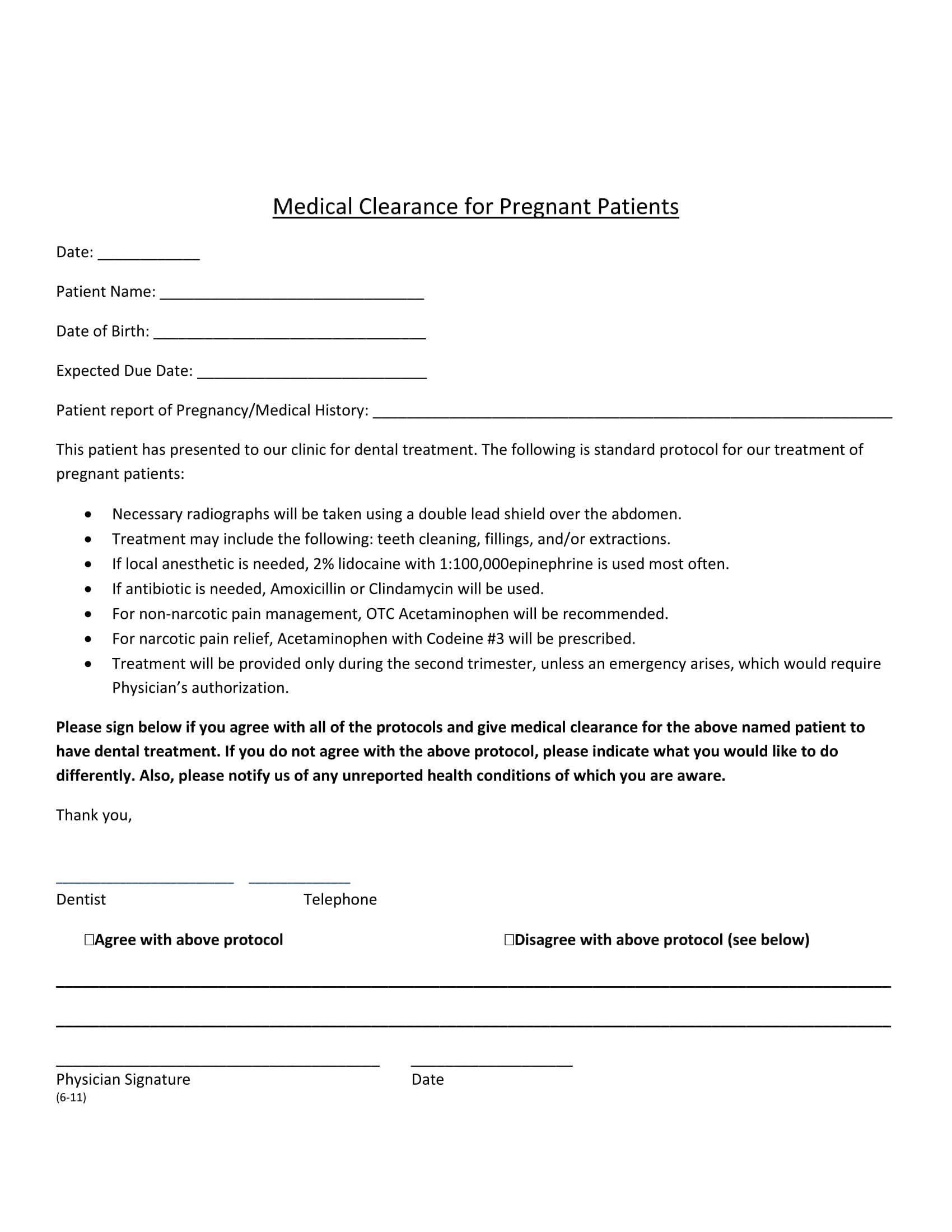
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Printable Medical Clearance Form For Dental Treatment
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
Sample Medical Clearance Forms (Dental, Surgery, Work, etc.)
Printable Medical Clearance Form For Dental Treatment
Printable Dental Medical Clearance Form
FREE 14+ Dental Medical Clearance Forms in PDF MS Word
FREE 31+ Medical Clearance Forms in PDF MS Word

Medical Clearance For Dental Treatment Audubon Dental Fill and
Web Physician Name (Please Print) Physician Signature Date We Appreciate Your Assistance In Providing Optimum Care For This Patient.
5 Star Ratedtrusted By Millions30 Day Free Trialcancel Anytime
We Appreciate Your Assistance In Providing.
Web Medical Clearance For Dental Treatment.
Related Post: