Printable Dental Claim Form
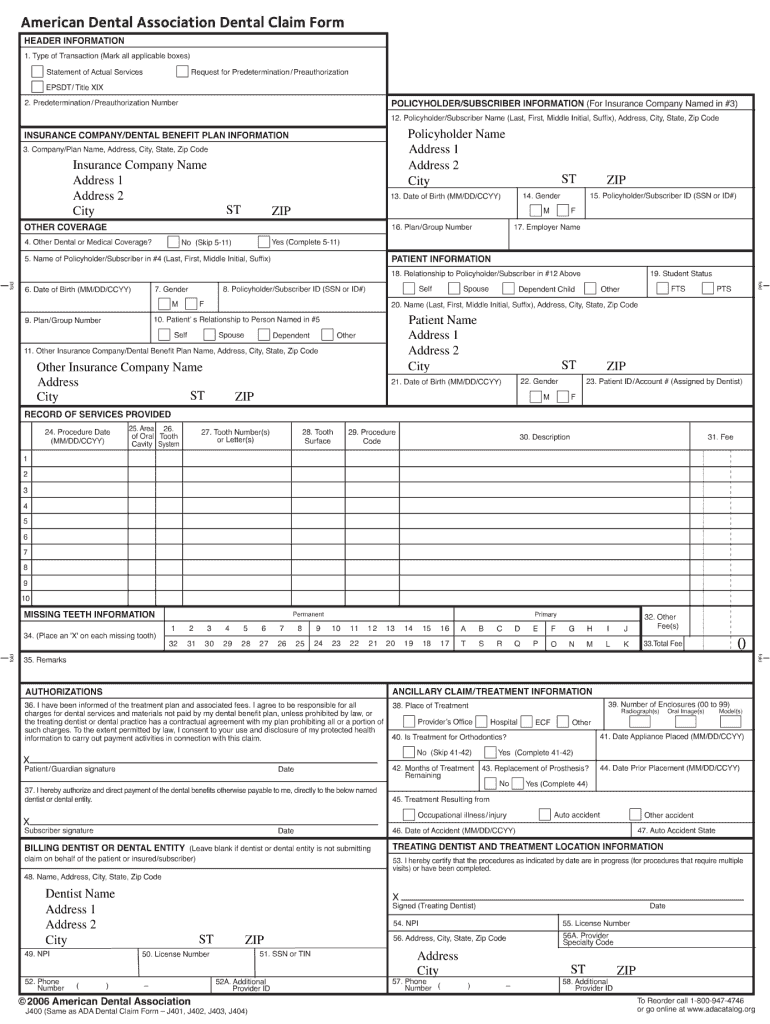
Printable Dental Claim Form - Get the forms you need today! Complete all information requested below. If none, leave blank.) record of services provided authorizations ancillary claim/treatment information. View, download and print dental forms. Web the ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d). The ada’s council on dental benefit programs has responsibility for electronic and paper dental claim content and completion instructions. Complete all items unless noted otherwise on the form or in the. Web access delta dental's administrative forms for dentists. Go to the forms page. Web dental forms & resources. Web ada dental claim form completion instructions. This area of the claim form provides information on the existence of additional dental or medical. Be certain to sign the authorization to release information in block 28. Find the forms and information you need. Web the ada dental claim form was revised in 2019 with editorial changes to form captions and check. If you wish to have your benefits for this claim paid directly to your dentist, sign block 29. Web ada dental claim form completion instructions version 2019 © american dental association page 1 of 16. Web please include the following to facilitate handling of your claim: Claim forms that can be customized, duplicated, imported, exported, or deleted. Ada policy promotes. If none, leave blank.) record of services provided authorizations ancillary claim/treatment information. Go to the forms page. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. The original claim form templates that come with open dental. Claim forms that can be customized, duplicated, imported, exported, or deleted. Complete all information requested below. Web access delta dental's administrative forms for dentists. Web the ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d). Web ada dental claim form completion instructions version 2019 ©. Trusted by millionsform search enginefast, easy & securefree mobile app If you wish to have your benefits for this claim paid directly to your dentist, sign block 29. You can complete and submit this form, or your dental provider can submit a claim on your behalf. Web access delta dental's administrative forms for dentists. Web ada dental claim form completion. Get the forms you need today! Web access delta dental's administrative forms for dentists. I have been informed of the treatment plan and associated fees. Benefit plan, unless the treating dentist or dental practice has a contractual agreement. Be certain to sign the authorization to release information in block 28. Web please include the following to facilitate handling of your claim: Web ada dental claim form completion instructions version 2019 © american dental association page 1 of 16. Web access delta dental's administrative forms for dentists. Claim forms that can be customized, duplicated, imported, exported, or deleted. The original claim form templates that come with open dental. Ada policy promotes use and acceptance of the most current version of the ada dental claim form by dentists and payers. If none, leave blank.) record of services provided authorizations ancillary claim/treatment information. Web dental forms & resources. Find the forms and information you need. Claim form (english) claim form (spanish) disputes and appeals. This is the most recent version of the form… If none, leave blank.) record of services provided authorizations ancillary claim/treatment information. Web the ada dental claim form provides a common format for reporting dental services to a patient's dental benefit plan. Claim form (english) claim form (spanish) disputes and appeals. Web please include the following to facilitate handling of your. Web forms & resources for dentists. With my plan prohibiting all or a portion of such charges. Web the ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d). The ada’s council on dental benefit. Claim form (english) claim form (spanish) disputes and appeals. Web the ada dental claim form was revised in 2019 with editorial changes to form captions and check box options for gender (m, f and u) to be consistent with the hipaa standard electronic dental claim (837d). Simplify paperwork and streamline processes. Find the forms and information you need. The ada’s council on dental benefit programs has responsibility for electronic and paper dental claim content and completion instructions. With my plan prohibiting all or a portion of such charges. If none, leave blank.) record of services provided authorizations ancillary claim/treatment information. If you wish to have your benefits for this claim paid directly to your dentist, sign block 29. I have been informed of the treatment plan and associated fees. This area of the claim form provides information on the existence of additional dental or medical. Web please include the following to facilitate handling of your claim: Applications and forms for dentists and their patients. Benefit plan, unless the treating dentist or dental practice has a contractual agreement. Complete all information requested below. Trusted by millionsform search enginefast, easy & securefree mobile app You can complete and submit this form, or your dental provider can submit a claim on your behalf.
Free Printable Ada Dental Claim Form
Fillable Delta Dental Claim Form Printable Forms Free Online
Fillable Dental Claim Form Printable Forms Free Online
Blank Printable Ada Dental Claim Form Printable Forms Free Online
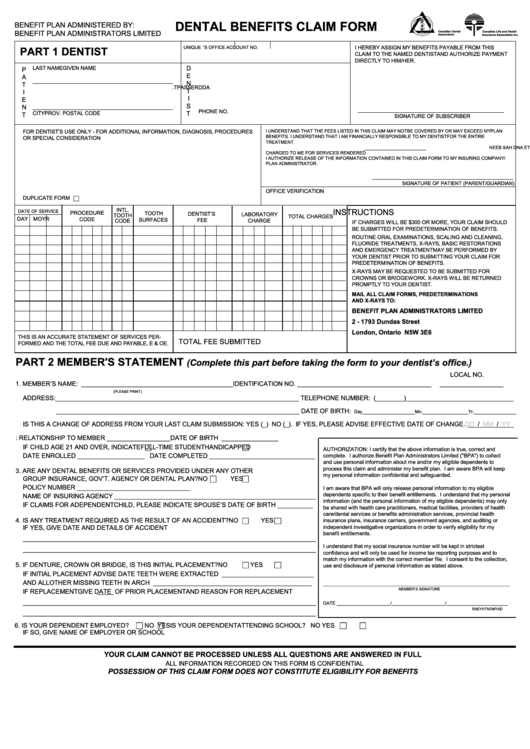
Fillable Dental Benefits Claim Form printable pdf download
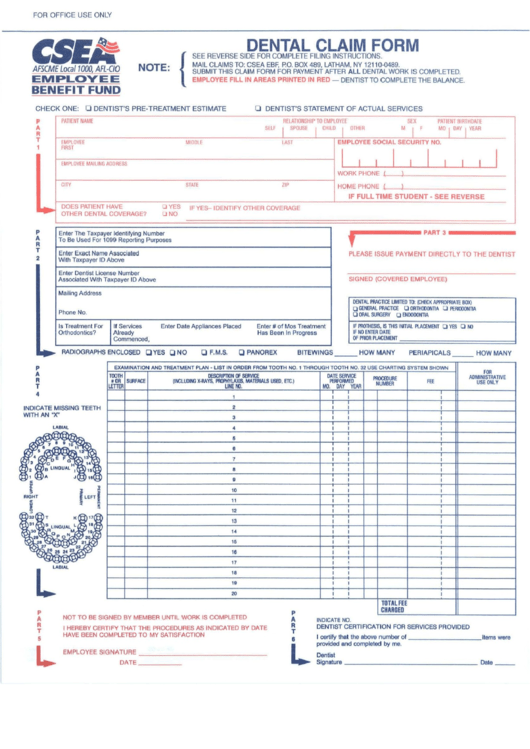
Fillable Csea Dental Claim Form printable pdf download
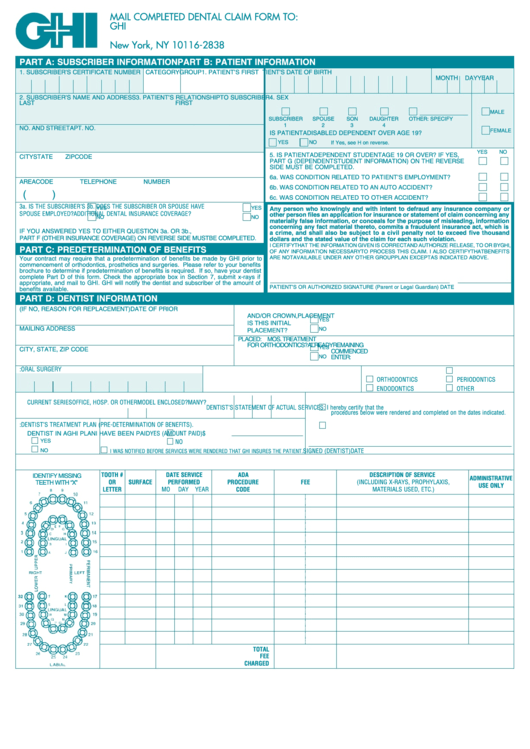
Form D437b Ghi Dental Claim Form printable pdf download

Dentist'S Claim Form printable pdf download
Printable Dental Claim Form 2018 Fill and Sign Printable Template

Physicians Mutual Insurance Company Dental Insurance Claim Form. Dental
Use Separate Form For Each Family Member And For Each Accident Or Illness.
Go To The Forms Page.
This Is The Most Recent Version Of The Form…
Claim Forms That Can Be Customized, Duplicated, Imported, Exported, Or Deleted.
Related Post: