Medicare Charting Examples
Medicare Charting Examples - Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. Describe resident’s ability to swallow foods and skilled nursing interventions used. Once the cert program identifies a claim in the sample, it requests (via fax, letter, or phone call) the Streamline your documentation process, ensure compliance, and elevate patient care effortlessly. Web section 30 in chapter 8 of the medicare benefit policy manual outlines factors for consideration in determining snf level of care, defines skilled services, and further lists principles for determining whether a service is skilled. For example, these include the following: Web common formats used to document patient care include charting by exception, focused dar notes, narrative notes, soapie progress notes, patient discharge summaries, and minimum data set (mds) charting. Web nursing staff must chart medicare a residents once every 24 hours. Document vitals, health status, and why the resident is receiving services. Web in this toolkit on simplified outpatient documentation, learn to describe the most recent billing and coding documentation guidelines, implement workflow solutions for more efficient documentation, and provide examples of documentation to help. For example, these include the following: Web medicare charting if a resident's primary payor source is medicare, nursing staff must document on the medical record once every 24 hours. For example if they had a hip fx your charting should really concentrate on the therapy they are doing, how they tolerate the therapy, pain, are they compliant with weight bearing. Web medicare does pay for a wellness visit once a year to identify health risks and help you to reduce them. For example, these include the following: Document vitals, health status, and why the resident is receiving services. For example if they had a hip fx your charting should really concentrate on the therapy they are doing, how they tolerate. Web describe exactly how the resident communicates and makes needs known. Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. They may also require documentation each shift. Centers for medicare & medicaid services. Web providers are responsible for documenting each patient encounter completely, accurately, and. Most facilities divide that charting between day and evening shifts. For example, these include the following: Web the centers for medicare & medicaid services (cms) evaluates mdm based upon the highest 2 of the following 3 elements: The charting should include vital signs, why the resident is receiving skilled services, and an excellent description of the resident's condition at that. Once the cert program identifies a claim in the sample, it requests (via fax, letter, or phone call) the Web nursing staff must chart medicare a residents once every 24 hours. For example, these include the following: Web unlike a straight narrative note, several types of nursing notes provide a structure for charting that aligns with the nursing process. Web. Web the centers for medicare & medicaid services (cms) evaluates mdm based upon the highest 2 of the following 3 elements: Describe resident’s ability to swallow foods and skilled nursing interventions used. Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. Document vitals, health status,. The number of diagnostic and management options to be considered; Web medicare does pay for a wellness visit once a year to identify health risks and help you to reduce them. Web key elements of medicare documentation. Web section 30 in chapter 8 of the medicare benefit policy manual outlines factors for consideration in determining snf level of care, defines. Because providers rely on documentation to communicate important patient information, incomplete and inaccurate documentation can result in unintended and even dangerous patient outcomes. Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. Web common formats used to document patient care include charting by exception, focused. Web providers are responsible for documenting each patient encounter completely, accurately, and on time. Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. Medicare benefit policy manual, chapter 8. Centers for medicare & medicaid services. Once the cert program identifies a claim in the sample,. The number of diagnostic and management options to be considered; Because providers rely on documentation to communicate important patient information, incomplete and inaccurate documentation can result in unintended and even dangerous patient outcomes. The charting should include vital signs, why the resident is receiving skilled services, and an excellent description of the resident's condition at that time. Describe resident’s ability. Describe skilled nursing interventions used to compensate for speech deficits. The charting should include vital signs, why the resident is receiving skilled services, and an excellent description of the resident's condition at that time. Medicare benefit policy manual, chapter 8. Web medicare charting if a resident's primary payor source is medicare, nursing staff must document on the medical record once every 24 hours. Find snfs in your area. At your wellness visit, our health care team will take a complete health history and. For example, if a thermal paper fax paper is used, a copy of it must be made for filing in the medical record since the print on thermal paper fades over time. They may also require documentation each shift. Web if fax records are maintained in the medical record, the facility must be sure that the record will maintain its integrity over time. Web under cert, we review a random sample of medicare ffs claims to determine if we paid them correctly under medicare coverage, coding, and billing rules. The number of diagnostic and management options to be considered; See different examples of nursing notes and discover tips to improve your documentation skills. Web is nurse charting the bane of your existence? Some facilities require a nurses note on medicare residents once each shift. Describe resident’s ability to swallow foods and skilled nursing interventions used. Web the centers for medicare & medicaid services (cms) evaluates mdm based upon the highest 2 of the following 3 elements: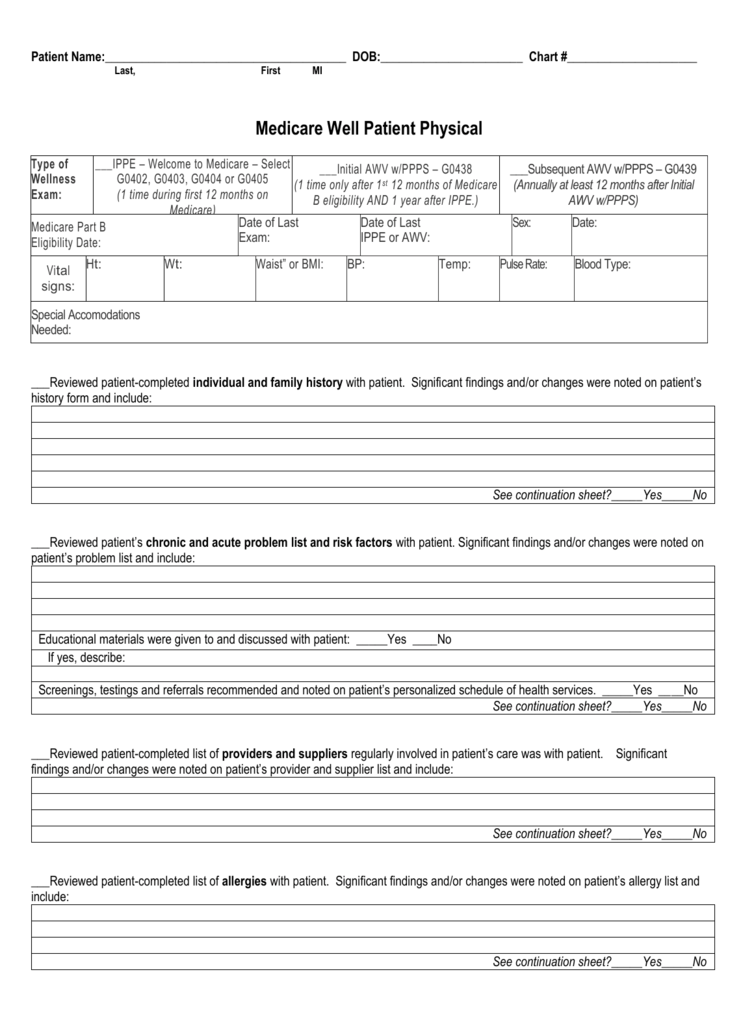
Medicare Charting Templates Master of Documents
Medicare Everything You Always Wanted to Know Wealthspire
Charting Guide Medicare (United States) Pain

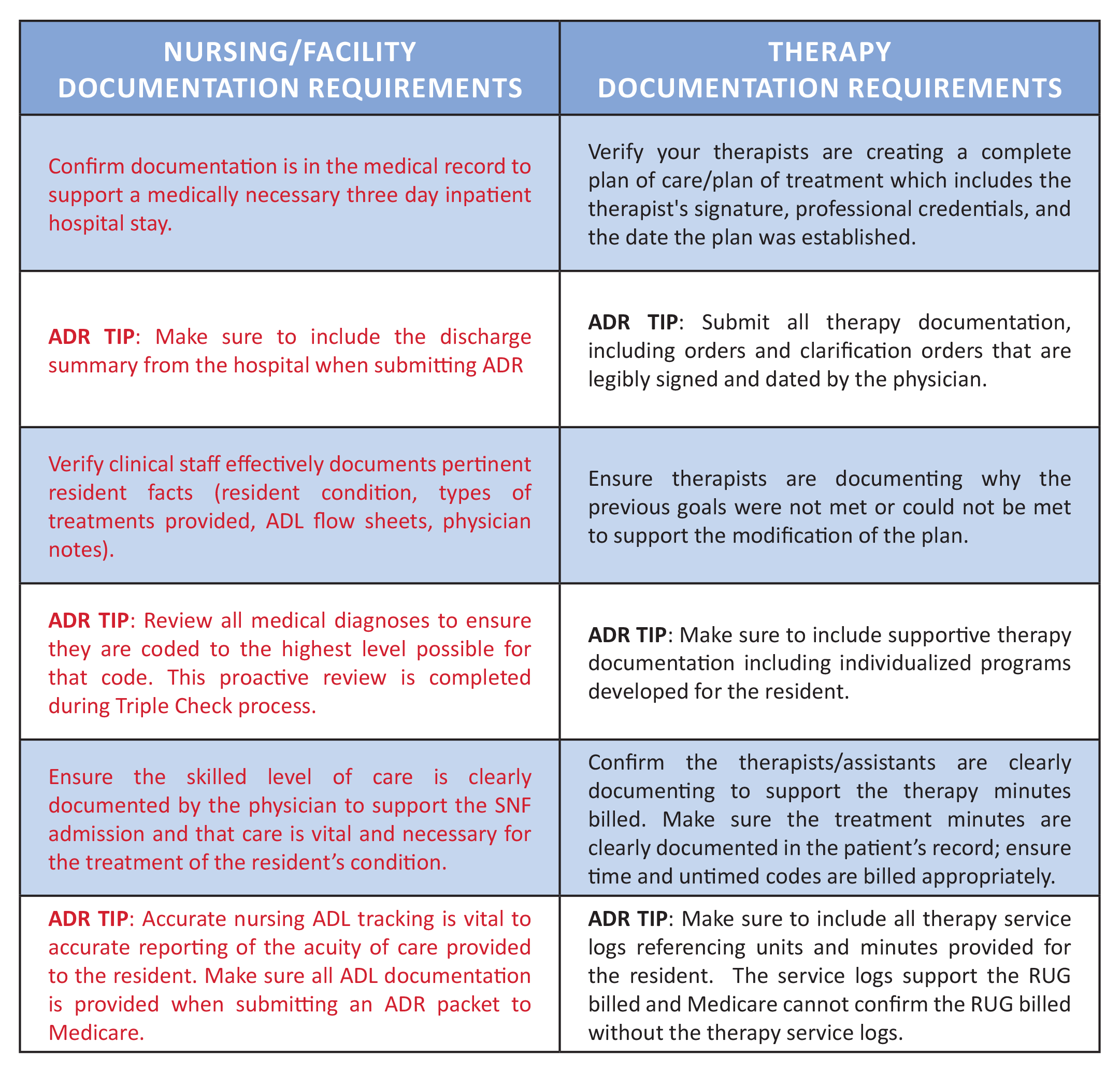
Examples of Documentation of Skilled and Unskilled Care for Medicare
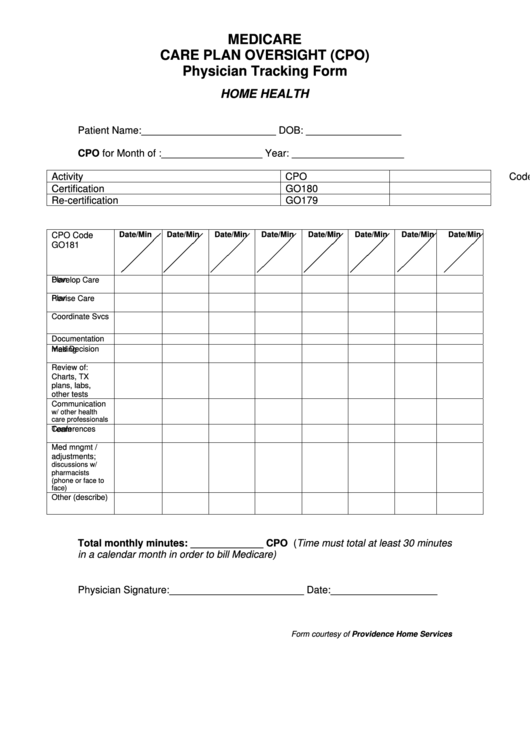
Medicare Care Plan Oversight Physician Tracking Form printable pdf
Medicare Eob Online For Providers Medicare Pathways

Medicare 8 Min Chart
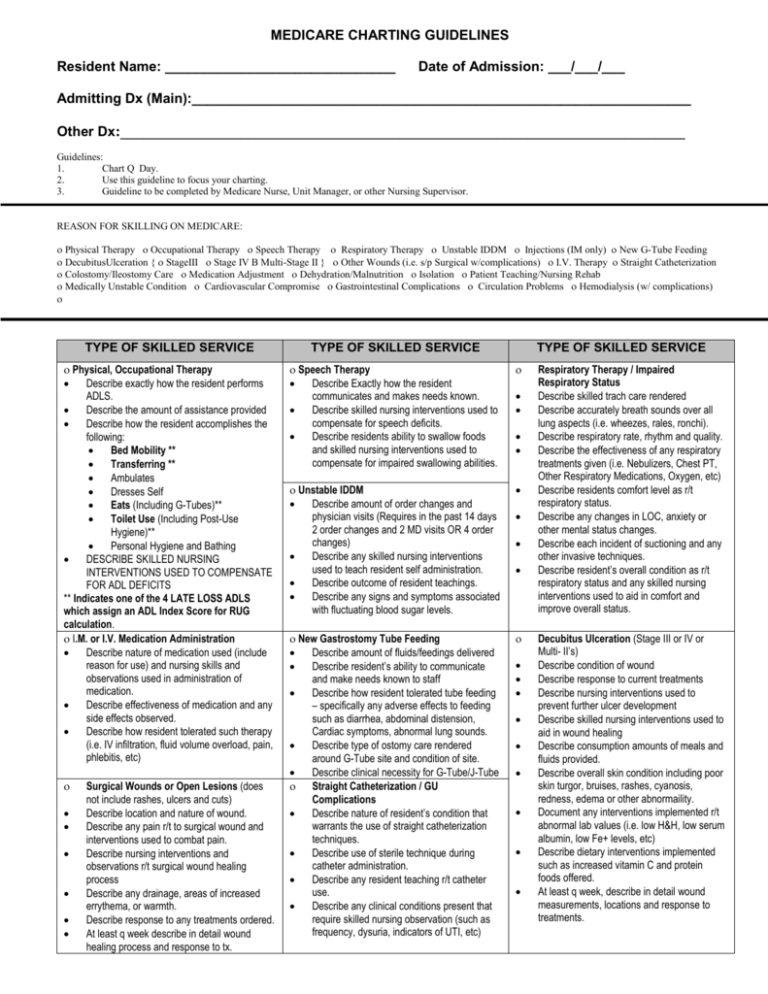
MEDICARE CHARTING GUIDELINES
How To Do Medicare Charting
The 2020 Medicare Documentation, Coding, and Payment Update AAFP
Once The Cert Program Identifies A Claim In The Sample, It Requests (Via Fax, Letter, Or Phone Call) The
Web Unlike A Straight Narrative Note, Several Types Of Nursing Notes Provide A Structure For Charting That Aligns With The Nursing Process.
Web Nursing Staff Must Chart Medicare A Residents Once Every 24 Hours.
Streamline Your Documentation Process, Ensure Compliance, And Elevate Patient Care Effortlessly.
Related Post:
