Form Cmsl564 Printable
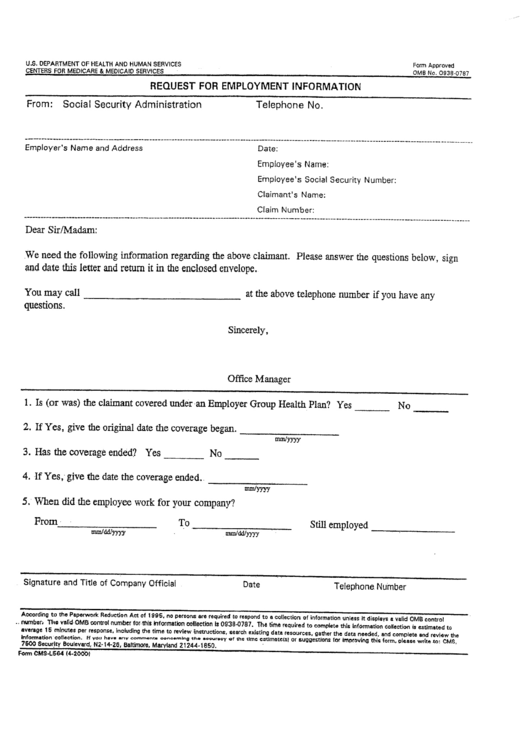
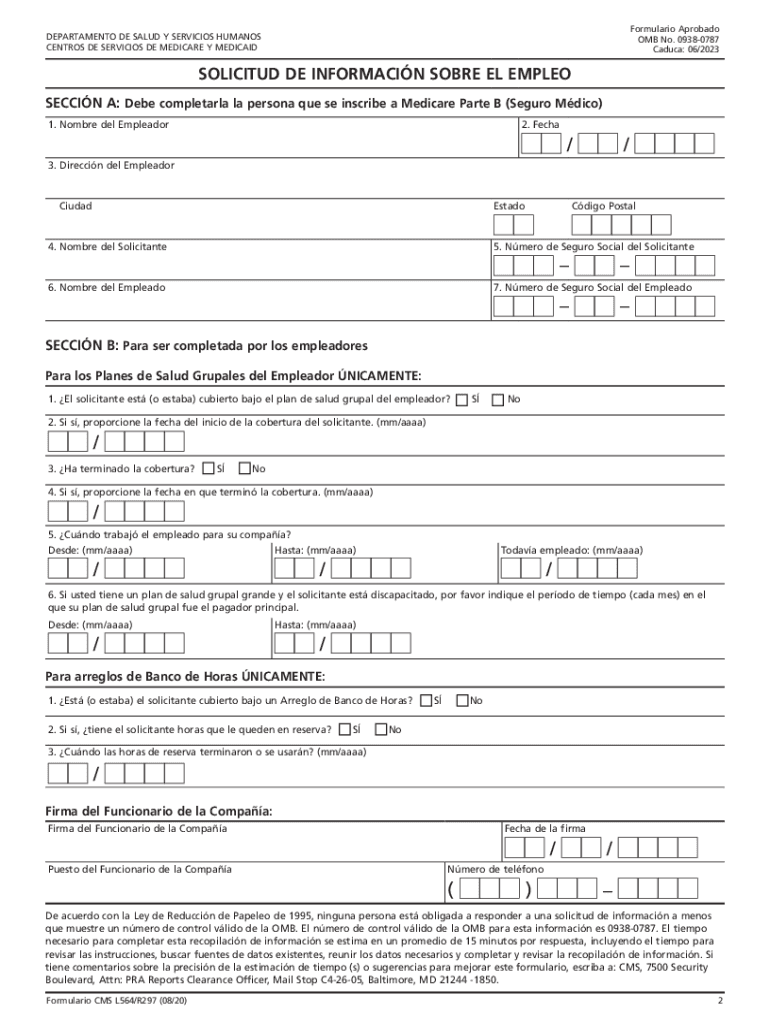
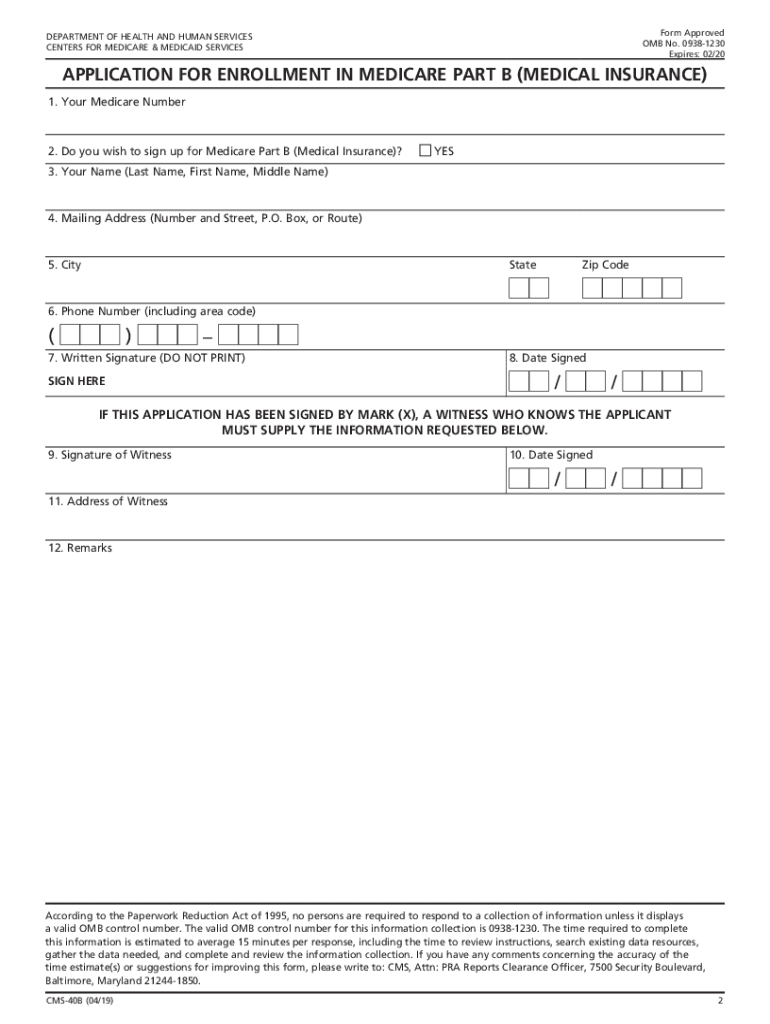
Form Cmsl564 Printable - You are responsible to fill out section a of this form with your employer’s name and address. Edit on any deviceform search enginefree mobile appcancel anytime Web this form is used for proof of group health care coverage based on current employment. Department of health and human services centers for medicare & medicaid services form approved omb no. Free mobile appsign on any devicetrusted by millionspaperless workflow The applicant completes section a and the employer, the ghp. This information is needed to process your medicare enrollment application. Web follow the simple instructions below: If you have a special situation, fill out the. Ask your employer to fill out section b. Web form cms l564/r297 is often used in u.s. You need to get the completed form from your employer and include it with your. Web follow the simple instructions below: Free mobile appsign on any devicetrusted by millionspaperless workflow If you have a special situation, fill out the. This information is needed to process your medicare enrollment application. You need to get the completed form from your employer and include it with your. Web form cms l564/r297 is often used in u.s. Legal, business, tax and other documents require a high level of compliance with the legislation and protection. You are responsible to fill out section a of. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. The applicant completes section a and the employer, the ghp. Web this form is used for proof of group health care coverage based on current employment. Department of health and human services centers for medicare. Department of health and human services centers for medicare & medicaid services form approved omb no. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. Legal, business, tax and other documents require a high level of compliance with the legislation and protection. Our forms. This information is needed to process your medicare enrollment application. Web this form is used for proof of group health care coverage based on current employment. Web fill out section a and take the form to your employer. Free mobile appsign on any devicetrusted by millionspaperless workflow The applicant completes section a and the employer, the ghp. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. Legal, business, tax and other documents require a high level of compliance with the legislation and protection. Web follow the simple instructions below: This information is needed to process your medicare enrollment application. Our forms. Legal, business, tax and other documents require a high level of compliance with the legislation and protection. If you have a special situation, fill out the. Ask your employer to fill out section b. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. Edit. This information is needed to process your medicare enrollment application. Web follow the simple instructions below: Legal, business, tax and other documents require a high level of compliance with the legislation and protection. If you have a special situation, fill out the. • if you’re in your iep and refused part b or did not sign up when you applied. Web this form is used for proof of group health care coverage based on current employment. • if you want to sign up for part b during the general. You are responsible to fill out section a of this form with your employer’s name and address. • if you’re in your iep and refused part b or did not sign. You need to get the completed form from your employer and include it with your. Our forms are updated on a. This information is needed to process your medicare enrollment application. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. Free mobile appsign on. Free mobile appsign on any devicetrusted by millionspaperless workflow Department of health and human services centers for medicare & medicaid services form approved omb no. Web follow the simple instructions below: This information is needed to process your medicare enrollment application. Web form cms l564/r297 is often used in u.s. You need to get the completed form from your employer and include it with your. • if you’re in your iep and refused part b or did not sign up when you applied for medicare, but now want part b. The applicant completes section a and the employer, the ghp. Web this form is used for proof of group health care coverage based on current employment. Our forms are updated on a. Ask your employer to fill out section b. Legal, business, tax and other documents require a high level of compliance with the legislation and protection. You are responsible to fill out section a of this form with your employer’s name and address.
Medicare Part B Application Form Cms L564 Universal Network

2005 Form CMS20031 Fill Online, Printable, Fillable, Blank pdfFiller
FREE 21+ Sample Application Forms in PDF MS Word Excel
Form CmsL564 Request For Employment Information printable pdf download

Medicare Enrollment Form Cmsl564 Enrollment Form
How to complete form 40b and l564 for your medicare part b enrollment?
Medicare Part B Enrollment Application Form DocHub
Medicare Form Cms L564 Printable Printable Forms Free Online
Medicare Form Cms L564 Printable Printable Forms Free Online
Fillable Form Cms671 Ltc Facility Application For Medicare/medicaid
Web Fill Out Section A And Take The Form To Your Employer.
Edit On Any Deviceform Search Enginefree Mobile Appcancel Anytime
• If You Want To Sign Up For Part B During The General.
If You Have A Special Situation, Fill Out The.
Related Post: